Diagnosis and Staging
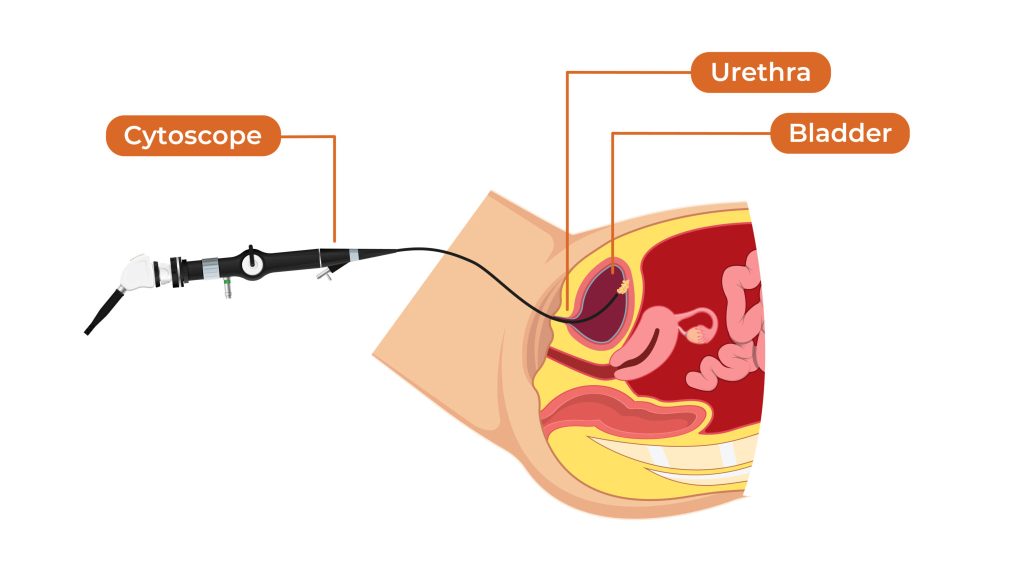
Diagnosis typically begins with urine tests (cytology, tumor markers), followed by cystoscopy — a key procedure where a thin, lighted scope is inserted through the urethra to directly visualize the bladder interior and identify tumors.
Here are visuals of cystoscopy showing a bladder tumor:
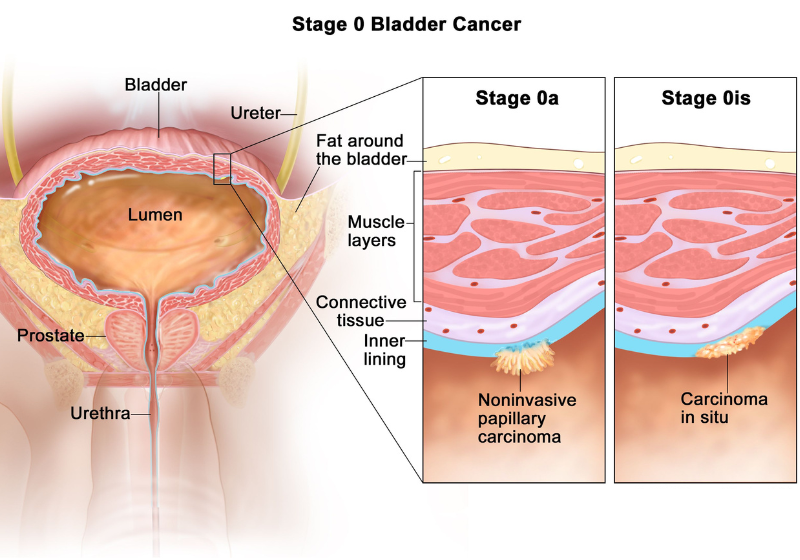
Bladder cancer is staged using the TNM system (Tumor, Node, Metastasis), from non-invasive (Ta, Tis, T1) to muscle-invasive (T2+) and advanced stages.
Treatment Approaches
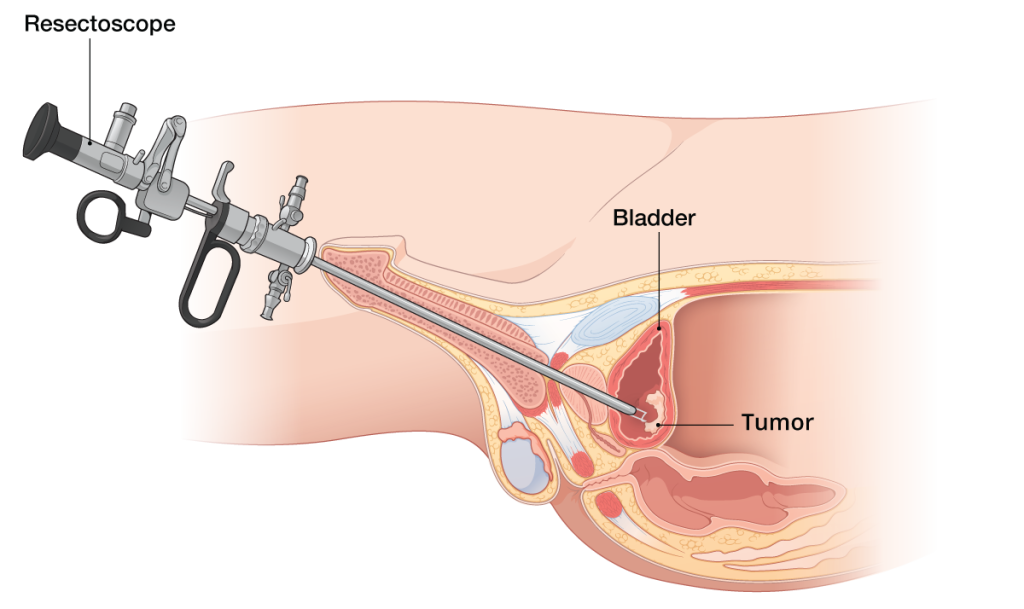
For non-muscle invasive bladder cancer, the primary treatment is transurethral resection of bladder tumor (TURBT) — endoscopic removal of the tumor through the urethra using a resectoscope.
Here are illustrations of the TURBT procedure:
After TURBT, intravesical therapy is often used to prevent recurrence: chemotherapy (e.g., mitomycin) instilled directly into the bladder, or immunotherapy with BCG (Bacillus Calmette-Guérin) for higher-risk cases.
For muscle-invasive bladder cancer, options include radical cystectomy (bladder removal with urinary diversion), chemotherapy, radiation, or bladder-preserving approaches (trimodality therapy). Advanced cases may involve systemic immunotherapy or targeted therapies.